摘要: 目的:探讨调脂方案对急性非心源性脑梗死合并脑微出血患者临床结局的影响。方法:连续回顾性纳入2016年1月1日~2021年2月28日在青岛大学附属医院住院的应用调脂药物的急性非心源性脑梗死合并脑微出血患者。根据调脂药物方案将患者分为常规降脂方案组及强化降脂方案组。对患者进行电话随访,采集患者出院后临床结局信息。应用Kaplan-Meier法及Cox回归分析对2组患者进行预后分析。结果:本研究共纳入268例患者:常规降脂方案组230例,强化降脂方案组38例。2组间人口统计学特征和血管危险因素的差异均无统计学意义(均P > 0.05)。强化降脂方案不会显著减少急性非心源性脑梗死合并脑微出血患者缺血性脑卒中复发风险(HR = 0.326, 95% CI 0.076~1.386; P = 0.129),不会显著增加此类患者自发性脑出血风险(HR = 2.087, 95% CI 0.124~20.393; P = 0.527),也不会显著减少此类患者全因死亡风险(HR = 0.752, 95% CI 0.171~3.312; P = 0.706)。结论:调脂方案不会影响急性非心源性脑梗死合并脑微出血患者脑卒中复发风险和全因死亡风险。
Abstract:
Objective: Our aim was to verify the impact of lipid-lowering therapy on the clinical outcomes of patients with acute non-cardiogenic cerebral infarction combined with cerebral microbleeds (CMBs). Methods: We conducted a single-centered, retrospective, observational cohort study of patients with acute non-cardiogenic cerebral infarction combined with CMBs and treated lipid-lowering therapy between Jan 1, 2016, and Feb 28, 2021 at the Affiliated Hospital of Qingdao University. According to the lipid-lowering therapy, patients were divided into a conventional lipid-lowering therapy group and an intensive lipid-lowering therapy group. During the follow-up period, we collected clinical outcome information after discharge by telephone. We drew Kaplan-Meier curves and constructed Cox proportional hazards regression models to verify the influence of different lipid regulation therapies in prognosis. Results: A total of 268 patients were finally included in this study: 230 in the conventional lipid-lowering therapy group and 38 in the intensive lipid-lowering therapy group. There was no statistically significant difference in demographic characteristics and vascular risk factors between the two groups (all P > 0.05). Intensive lipid-lowering therapy did not significantly reduce the risk of ischemic stroke recurrence in patients with acute non-cardiogenic cerebral infarction combined with CMBs (HR = 0.326, 95% CI 0.076~1.386; P = 0.129). Intensive lipid-lowering therapy also could not significantly increase the risk of intracerebral hemorrhage (HR = 2.087, 95% CI 0.124~20.393; P = 0.527) and reduce the risk of all-cause death (HR = 0.752, 95% CI 0.171~3.312; P = 0.706). Conclusion: The lipid-lowering therapy would not influence the recurrent stroke rate and all-cause mortality in patients with acute non-cardiogenic cerebral infarction combined with CMBs.
1. 引言
脑微出血是脑小血管病(cerebral small vessel disease, CSVD)的影像学标志物之一,是由于脑小血管病变导致血液成分(如含铁血黄素)外渗至血管周围间隙所致,在T2加权成像或磁敏感加权成像(susceptibility-weighted imaging, SWI)上表现为小圆形低密度灶,直径 < 10 mm [1] [2] 。在既往无脑血管病的患者中,脑微出血的检出率约5% [3] ,在缺血性脑卒中患者中脑微出血检出率为35%~71% [4] 。既往研究发现脑微出血与脑卒中后的缺血性脑卒中复发、脑出血和死亡风险相关 [5] [6] [7] 。
低密度脂蛋白是脑卒中的危险因素 [8] ,既往研究表明应用他汀类药物降低患者1 mmol/l血低密度脂蛋白可降低大约21.1%的脑卒中风险 [9] 。调脂药物是脑梗死患者二级预防的重要组成部分。调脂药物的应用是否会增加脑微出血的风险目前尚且存在争议。在一项颅脑磁共振随机对照试验的亚组研究中,研究者发现瑞舒伐他汀的应用不会增加脑微出血的风险 [10] ,而且阿托伐他汀短期降脂治疗同样对脑微出血的产生没有明显影响 [11] 。但是,在急性脑出血人群中(不论是自发性脑出血 [12] 还是抗凝药相关脑出血 [13] 患者),研究者得出了与之相矛盾的结论,他们发现他汀类药物的应用与新发脑微出血或增加脑微出血负荷相关。鉴于目前对于调脂药物与脑微出血的关系尚无定论,在此我们对急性非心源性脑梗死合并脑微出血患者调脂药物的应用与临床结局的相关性进行分析,以进一步指导合并脑微出血的脑梗死患者调脂药物的应用。
2. 对象与方法
2.1. 研究对象
本研究回顾性分析青岛大学附属医院2016年1月1日~2021年2月28日连续住院的应用调脂药物的急性非心源性脑梗死合并脑微出血患者268例。本研究由于回顾性且不干预患者治疗,已通过医院伦理委员会的知情同意豁免批准(伦理号QYFY WZLL 27297)。
2.1.1. 纳入标准
(1) 年龄大于18周岁;(2) 在症状出现48小时内入院的急性脑梗死患者,脑梗死由脑MRI检查证实,符合《中国急性缺血性卒中诊治指南2018》 [14] 的诊断标准;(3) 非心源性脑梗死依据脑卒中病因TOAST分型 [15] 诊断,包括大动脉粥样硬化型和小动脉闭塞型;(4) 经SWI扫描证实脑微出血的存在,脑微出血的诊断标准参考《中国脑小血管病诊治共识》 [1] ;(5) 应用调脂药物治疗。
2.1.2. 排除标准
(1) 合并急性脑出血、蛛网膜下腔出血或急性脑梗死后出血转化;(2) 合并严重的心、肺、肝、肾功能衰竭或昏迷,凝血功能异常、恶性肿瘤晚期或者严重血液病;(3) 接受溶栓治疗或抗凝治疗;(4) 停用降脂药物治疗。
2.2. 方法
我们收集了纳入患者的以下临床资料:年龄、性别、吸烟史、饮酒史、既往史(高血压、糖尿病、冠心病)、甘油三酯、低密度脂蛋白。所有患者出院后常规给予脑梗死二级预防治疗,根据调脂药物方案将患者分为常规降脂方案组和强化降脂方案组。患者的降脂方案取决于其主治医师的决定。常规降脂方案指仅使用一种中等强度他汀类药物。强化降脂方案指增加他汀类药物的剂量或应用2种及以上调脂药物,以1.8 mmol/l为低密度脂蛋白达标值或以降低低密度脂蛋白50%为目标的强化降脂方案。强化降脂治疗维持时间大于3个月,后续继续降脂治疗,后续降脂方案取决于其复诊时主治医师的决定。降脂药物包括:阿托伐他汀、瑞舒伐他汀、依折麦布等。以常规调脂方案组为对照组,分析强化降脂方案组与急性非心源性脑梗死合并脑微出血患者临床结局的相关性。终点事件为复发性缺血性脑卒中,其他结局包括自发性脑出血、全因死亡。缺血性脑卒中复发定义为快速出现的新的局灶性神经功能缺损,有缺血性脑卒中的临床或影像学证据,或者是现有局灶性神经功能缺损的迅速恶化。我们对纳入患者进行随访,直到出现以下事件之一:(1) 复发性缺血性脑卒中(终点事件);(2) 自发性脑出血;(3) 全因死亡;(4) 试验终止(2022年5月31日)。
2.3. 统计学方法
使用IBM SPSS 25以及GraphPad Prism 9.0进行统计分析。将2组患者的基线资料绘制成表格,计量资料符合正态分布以平均数±标准差(χ ± s)表示,采用独立样本t检验,计数资料以例(率)表示,采用卡方检验。绘制2组患者终点事件累计风险曲线,采用Log Rank检验,应用Cox回归分析计算风险比(hazard ratio, HR)和95%置信区间(confidence interval, CI)。再构建多因素Cox回归模型分析基线资料对临床结局差异的影响。P < 0.05,差异具有统计学意义。
3. 结果
在2016年1月1日至2021年2月28日期间,共268例急性非心源性脑梗死合并脑微出血患者纳入研究(见图1)。2组患者的基线资料特征见表1。本研究患者的平均年龄为65.86 ± 10.25岁,其中≥65岁146例(54.48%),男性179例(66.79%)。2组患者性别、年龄的差异无统计学意义(P > 0.05),2组患者吸烟史、饮酒史、高血压、糖尿病、冠心病、甘油三酯、低密度脂蛋白的差异均无统计学意义(P > 0.05) (见表1)。
随访期间共发生复发性缺血性脑卒中42例,其中常规降脂方案组40例(17.39%),强化降脂方案组2例(5.26%),强化降脂方案组缺血性脑卒中复发风险低于常规降脂方案组,但2组间差异无统计学意义(HR = 0.326, 95% CI 0.076~1.386; P = 0.129) (见图2和表2)。年龄 ≥ 65岁(HR = 2.547, 95% CI 1.213~5.352; P = 0.014)和甘油三酯 ≥ 1.7 mmol/l (HR = 2.391, 95% CI 1.195~4.782; P = 0.014)会增加急性非心源性脑梗死合并脑微出血患者复发性缺血性脑卒中风险(见图3)。

Table 1. Baseline characteristics of the study population
表1. 研究患者的基线资料
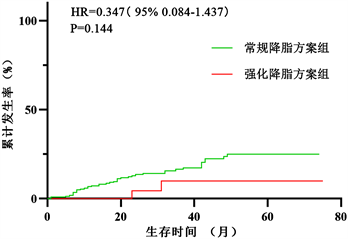
Figure 2. Cumulative risk curve of the endpoint between the conventional lipid-lowering therapy group and the intensive lipid-lowering therapy group
图2. 常规降脂方案组与强化降脂方案组终点事件累积风险曲线
随访期间共发生自发性脑出血6例,其中常规降脂方案组5例(2.17%),强化降脂方案组1例(2.63%),强化降脂方案组自发性脑出血风险较常规降脂方案组高,但2组间差异无统计学意义(HR = 2.087, 95% CI 0.124~20.393; P = 0.527) (见表2)。随访期间共发生全因死亡25例,其中常规降脂方案组22例(9.57%),强化降脂方案组3例(7.89%),强化降脂方案组全因死亡风险较常规降脂方案组低,但2组间差异无统计学意义(HR = 0.752, 95% CI 0.171~3.312; P = 0.706) (见表2)。
4. 讨论
本研究结果显示,两组患者在基线资料的差异上无统计学意义,具有可比性,由此可知,患者的共
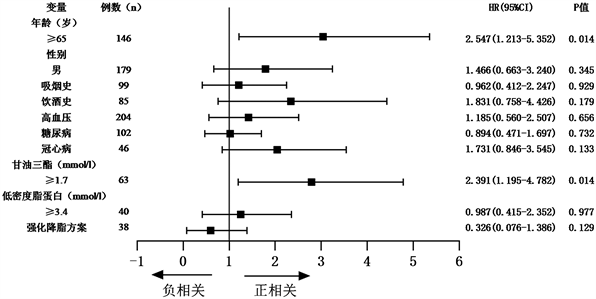
Figure 3. COX proportional hazards regression analysis of the endpoint
图3. 终点事件的COX比例风险回归分析
Table 2. COX regression analyses of risk of clinical outcomes between the conventional lipid-lowering therapy group and the intensive lipid-lowering therapy group
表2. 常规降脂方案组与强化降脂方案组临床结局风险的COX回归分析
#为年龄、性别、吸烟史、饮酒史、高血压、糖尿病、冠心病、甘油三酯、低密度脂蛋白。
病史及相关影像学结果并没有影响临床医生为患者制定调脂方案时的决策。与应用常规调脂方案的患者相比,应用强化降脂方案的患者在缺血性脑卒中复发、自发性脑出血、全因死亡的风险上没有明显增减。因此本研究考虑降脂方案的选择对急性非心源性脑梗死合并脑微出血患者的预后没有显著影响。既往研究表明低密度脂蛋白异常可能与轻型脑卒中及高危短暂性脑缺血发作人群发生脑梗死密切相关 [16] 。另有研究发现对于老年高危型脑梗死患者,强化降脂方案是较为安全的,且不增加患者脑微出血的个数 [17] 。但也有研究表明,脑梗死急性期较低的低密度脂蛋白水平可能与急性脑梗死出血性转化相关 [18] 。因此在脑梗死急性期可能强化降脂方案并不适用。我们的研究也有许多不足。本研究是单中心回顾性研究,并且鉴于样本量的不足,我们没有对患者依据年龄进一步分组,但有研究显示高龄与脑微出血的存在及不良结局相关 [19] 。此外我们没有对患者根据脑梗死部位、脑微出血的数量及部位进行进一步深入分析,这些因素都可能影响缺血性脑卒中复发风险,未来还需要更大的样本量及多中心前瞻性研究进一步分组以分析调脂药物方案对脑梗死合并脑微出血患者预后的影响。在我们的研究中,调脂药物的应用是由患者的主治医师自行评估决定,且患者应用不同降脂方案的时间不固定,可能与随机原则相悖并影响试验结果。因此未来需要大型研究以发现脑梗死合并脑微出血患者最适宜的调脂方案,以达到脑梗死复发与出血风险的最小化。
5. 结论
对于急性非心源性脑梗死合并脑微出血的患者,与常规降脂方案相比,强化降脂方案并没有明显影响缺血性脑卒中复发风险。未来需要更多的前瞻及干预性研究,以评估不同降脂方案对非心源性脑梗死合并脑微出血患者临床结局的影响。