1. 引言
胸腰椎爆裂性骨折(TLBF)常造成脊髓神经功能障碍和脊柱不稳而需要手术治疗 [1] ,目前经骨折椎骨置椎弓根钉内固定(Pedicle Screw Fixation at Fracture Vertebrae, PFFV)因良好的骨折复位和固定的效果已成为常用术式 [2] 。横连(Cross Link, CL)是脊柱内固定装置中常见的器械,通过连接两侧纵棒进而将两侧椎弓根钉纵棒连接成一体,横连常呈现1字型 [3] 。
但是目前对于横连在临床中的使用仍存在争议。部分研究表明横连能够增加内固定的稳定性,Lin H等人 [4] 认为:横连对于多节段PLIF具有良好的抗扭转的作用;Lei M等人 [5] 认为,在PE-PLIF使用新型双弯杆结构横连具有更好的生物力学性能;Mina A等人 [6] 认为,使用X型横连和长节段固定治疗胸腰椎爆裂性骨折可以达到良好的固定效果。Tianhao W等人 [7] 认为,横连降低脊柱截骨后长节段固定轴向旋转的活动度,且可以分散应力,应在截骨部位和近端段放置2个横连。Simone B等人 [8] 认为交联杆的使用增强了短节段固定的稳定性,使其在横向弯曲和轴向旋转中显着变硬,并限制在椎弓根螺钉松动时的运动。Farhad M等人 [9] 认为增加横连可以使创伤性胸腰椎骨折的患者有更好的融合效果和和患者临床满意度。
但仍有研究表明横连对于内固定稳定性作用不大,在青少年特发性脊柱侧凸的研究中发现,横连并不能改善脊柱后路融合术的临床和影像学指标 [10] [11] [12] 。Usmani MF等人 [13] 认为有无横连在脑瘫相关脊柱侧凸脊柱后路融合术中在实现矫正程度矫正维持率和并发症发生率方面无显著差异。Arvind G等人 [14] 认为不使用横连并不会造成扭转时的不稳定,因此在临床实践中横连是不需要使用的。Frédéric C等人 [15] 认为横连在多数情况下提供一些额外的轴向旋转稳定性,但是横向弯曲和屈曲受到影响较少,且临床发现横连强化只推荐于C1/C2节段。
随着经伤椎置钉固定在胸腰椎爆裂骨折中的应用,是否需要放置横连成为外科医师的疑点。伤椎椎弓根钉阻隔了棘间放置横连的空间,术中外科医师可以选择咬除部分棘突以放置横连,这破坏了棘上韧带,或者在棘突上打孔放置横连,这保护了棘突外形和棘上韧带的完整。但目前仍未见针对上述内固定方式稳定性的生物力学研究。因此本研究通过构建3种不同骨折内固定模型,以及取出内固定后脊柱模型,模拟日常的活动,评价脊柱的稳定性和安全性,研究胸腰椎爆裂骨折经伤椎置钉后是否需要横连,如果需要应该如何放置横连。
2. 材料和方法
2.1. 胸腰椎模型的建立
选择一名健康志愿者,使用CT机扫描其胸腰段,将图像以DICOM格式导入MINICS中进行椎体提取,导入GEOMAGIC中进行光顺处理和拟合曲面,导入SILIDWORKS中进行皮质骨松质骨的组装和椎间盘关节软骨的构建,由此构建出如图1(a)的T12-L2的脊柱模型。
2.2. 胸腰椎爆裂骨折模型的构建
使用V字型截骨截除L1椎体前中柱的部分骨质,并分割骨折上方骨质,造成脊柱前中柱的不连续,模拟爆裂骨折不稳的情况,如图1(b)。复位后椎体前缘压缩40%,脊柱后凸矫正角10˚并伴有上方骨质的破碎,根据脊柱载荷分享评分 [16] 为6分,可仅行后路固定。

Figure 1. Thoracolumbar spine and burst fracture model. (a) Complete spine model; (b) Burst fracture model
图1. 胸腰椎脊柱和爆裂骨折模型。(a) 完整脊柱模型;(b) 爆裂性骨折模型
2.3. 胸腰椎爆裂骨折内固定
构建经棘突放置横连内固定、切除棘突放置横连内固定和无横连内固定的经伤椎固定的胸腰椎爆裂骨折内固定模型,其中椎弓根钉长度为45 mm直径为6 mm,置钉平行于下终板且在椎弓根内。经棘突放置横连的空洞稍微大于横连的截面,而切除棘突仅需要切除放置横连的部分阻隔的棘突,同时构建了上述模型骨折愈合良好去除内固定装置后的脊柱模型,包括经棘突胸腰椎、切除棘突胸腰椎和完整胸腰椎模型,如图2所示。
构建TLBF固定于骨折椎体的内固定模型,包括经棘突放置横连内固定(TSPC)、切除棘突放置横连内固定(ESPC)和无横连内固定(NC)。椎弓根螺钉长度45 mm,直径6 mm。螺钉放置于与下终板平行的椎弓根内。经棘突放置横连的空洞稍微大于横连的截面,而切除棘突仅需要切除放置横连的部分阻隔的棘突,同时,构建骨折愈合良好内固定装置取出后的3种脊柱模型,包括经棘突横联去除(Through Spininous Process Cross-link Removed, TSPCR)、切除棘突横联去除(Excision Spininous Process Cross-Link Removed, ESPCR)和完整(No Cross-Link Removed, NCR)胸腰椎模型,如图2所示。

Figure 2. Different internal fixation and spine models. (a) TSPC; (b) ESPC; (c) NC; (d) TSPCR; (e) ESPCR; (f) NCR
图2. 不同的内固定和脊柱模型。(a) TSPC;(b) ESPC;(c) NC;(d) TSPCR;(e) ESPCR;(f) NCR
2.4. 力的加载
将上述模型导入ANSYS中,按照表1进行材料属性的设定,按照松质骨2 mm、皮质骨纤维环髓核内固定1.5 mm、终板和关节软骨1 mm的大小进行网格划分。按照表2使用非线性弹簧模拟椎旁韧带,其中切除棘突放置横连的模型因切除棘上韧带的起止点而破坏了棘上韧带,经棘突放置横连无棘上韧带的破坏,网格划分及椎旁韧带效果如图3示。对6种脊柱模型,固定L2椎体下表面,在T12椎体上表面给予500 N垂直向下的重力和10 Nm的扭矩,模拟前屈后伸侧屈扭转的运动。
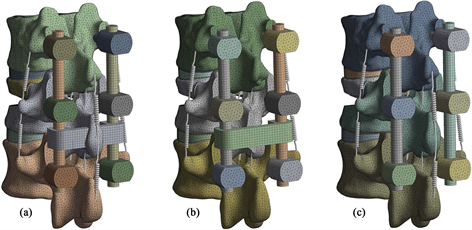
Figure 3. Mesh generation and paraspinal ligament. (a) TSPC; (b) ESPC; (c) NC
图3. 网格划分和椎旁韧带。(a) TSPC;(b) ESPC;(c) NC

Table 1. Material properties of different structures
表1. 不同结构的材料性质
Table 2. Stiffness values of different ligaments
表2. 不同韧带的强度值
2.5. 数据的收集和统计
对T12上表面位移较大的区域选择6个远程点,收集不同运动状态下远程点的位移和活动度,收集T12、L1、L2椎弓根钉和纵棒的等效应力。不同脊柱模型的位移和活动度对比使用两独立样本t检验,α < 0.05差异具有统计学意义。
3. 结果
3.1. 有效性验证
固定胸腰椎模型L2椎体下表面,在T12上表面给予200 N垂直向下的外力和7.5 Nm的扭矩,收集不同状态下的活动度。将本研究和体外实验 [17] [18] 和既往有限元研究 [19] 对比如图4,在不同活动状态下活动度均在既往参考范围内,因此本模型可以用于下一步的研究。
3.2. 横连对模型位移的影响
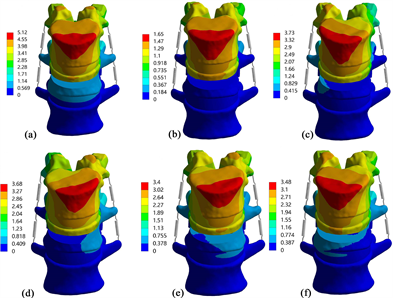
Figure 5. The displacement nephogram of TSPC. (a) flexion; (b) extension; (c) left bending; (d) right bending; (e) left torsion; (f) right torsion
图5. TPSC的位移云图。(a) 前屈;(b) 后伸;(c) 左屈;(d) 右屈;(e) 左扭转;(f) 右扭转
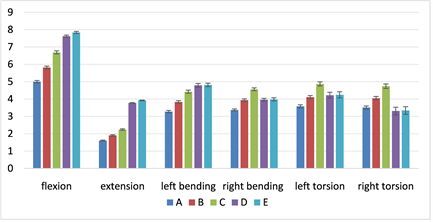
Figure 6. The displacement of different models under different motions. (a) TSPC; (b) ESPC; (c) NC; (d) TSPCR & NCR; (e) ESPCR
图6. 不同模型在不同活动状态下的位移。(a) TSPC;(b) ESPC;(c) NC;(d) TSPCR & NCR;(e) ESPCR
在6种活动状态下,不同脊柱内固定模型的位移从大到小为无横连 > 无棘突横连 > 棘突横连,差异具有统计学意义。无棘突横连较无横连在前屈后伸左侧屈右侧屈左扭转和右扭转时位移平均值分别减少了:13%、15.18%、13.35%、13.6%、15.61%、14.56%;棘突横连较无横连分别减少了:25.26%、28.57%、26.02%、26.1%、26.49%、25.95%。在去除内固定后,无横连和棘突横连因棘突完整拥有相同的位移和活动度。完整棘突和无棘突横连的术后对比中可见,在前屈后伸的活动中,无棘突横连的位移大于完整棘突,分别增加了2.89%和3.7%,差异具有统计学意义,在其他活动中差别无统计学意义。在位移云图中可见,位移最大位置出现在椎体前表面和上表面的交界处(见图5和图6)。
3.3. 横连对模型活动度的影响
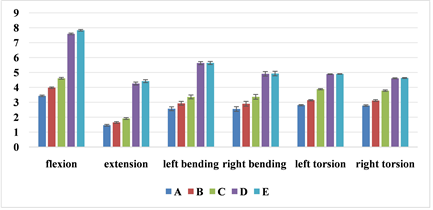
Figure 7. The ROM of different models under different motions. (A) TSPC; (B) ESPC; (C) NC; (D) TSPCR & NCR; (E) ESPCR
图7. 不同模型在不同活动下的活动度。(A) TSPC;(B) ESPC;(C) NC;(D) TSPCR & NCR;(E) ESPCR
横连对内固定活动度的影响和对位移的影响类似,活动度在横连棘突内固定中最小,而在无横连内固定中最大,无棘突横连较无横连在六种运动时位移平均值分别减少了:13.67%、13.61%、12.8%、13.95%、19.07%、17.46%;棘突横连较无横连分别减少了25.6%、23.56%、23.51%、24.33%、27.58%、26.46%。去除内固定后,无棘突横连内固定在前屈后伸时活动度大于完整棘突,分别增加了3.16%和3.76% (图7)。
3.4. 横连对内固定等效应力的影响
棘突横连内固定较无横连内固定降低了上位椎体和下位椎体椎弓根钉的等效应力,对骨折椎体椎弓根钉应力影响较小,增加了纵棒的等效应力(图8)。在应力云图中可见,椎弓根钉最大等效应力发生在椎弓根钉的根部,在纵棒中发生在纵棒和横连的连接处或纵棒和椎弓根钉连接处(图9)。

Figure 8. The effect of CL on the equivalent stress of internal fixations. (a) Upper vertebral pedicle screw; (b) Fractured vertebral pedicle screw; (c) Lower vertebral pedicle screw; (d) Connecting rod. A: TSPC, B: ESPC, C: NC
图8. 横连对内固定等效应力的影响。(a) 上位椎体椎弓根钉等效应力;(b) 骨折椎体椎弓根钉等效应力;(c) 下位椎体椎弓根钉等效应力;(d) 纵棒等效应力。A:横连棘突内固定,B:无棘突横连内固定,C:无横连内固定
4. 讨论
经伤椎置钉短节段固定对于治疗胸腰椎爆裂性骨折具有良好的治疗效果,但在临床中对于横连的作用存有争议,本研究首次通过医学有限元的方法,研究横连在经伤椎置钉短节段固定治疗胸腰椎爆裂骨折中的作用,研究表明:经棘突放置横连可以在不破坏脊柱后方复合体的前提下完成横连的放置,且内固定整体的位移和活动度最小,稳定性最高,放置横连在降低了临近椎体椎弓根钉的等效应力,使内固定更加安全。
经伤椎置钉固定后在需要放置横连的区域有棘突的阻隔,因此放置时常采用钻孔放置或者咬除一定棘突进行放置,但在跨伤椎置钉时,骨折椎体和临近椎体的棘突间有间隙,可以通过间隙放置横连,在对于短节段固定治疗胸腰椎骨折的体外实验中发现,无论在跨伤椎还是经伤椎固定中,放置横连提高了轴向旋转时稳定性 [20] 。本研究发现横连同样能够增加屈伸和侧屈时的稳定性。在研究横连在跨伤椎多阶段固定中作用的体外实验中,比较穿过棘突底部的横连、穿过棘突间的横连和无横连的3种内固定形式,研究表明:穿过棘突底部的横连增加了拉拔和屈曲压缩中的机械阻力,且在屈曲压缩时提供更强的抗中柱的损害能力 [21] 。本研究通过有限元的方法证明在穿过棘突放置横连能够增加在6种运动状态下的稳定性。
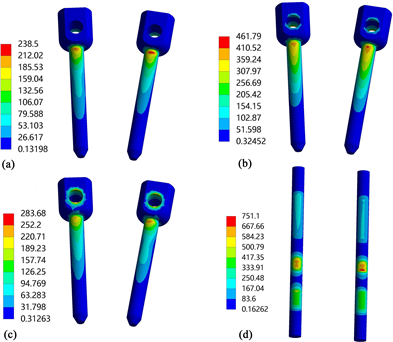
Figure 9. The equivalent stress nephogram of internal fixations of TSPC; (a) upper vertebral pedicle screw; (b) fractured vertebral pedicle screw; (c) lower vertebral pedicle screw, (d) connecting rod
图9. TSPC内固定物等效应力云图。(a) 上椎弓根螺钉;(b) 骨折椎弓根螺钉;(c) 下椎弓根螺钉;(d) 纵棒
在对于横连对创伤性胸腰椎骨折融合率和满意度的一项随机临床试验中发现:横连促进了胸腰椎骨折患者的融合率和治疗效果 [9] 。本研究发现穿过棘突放置横连在不破坏椎旁韧带的同时进一步增加了内固定的稳定性,稳定性的增加有助于术后融合率的增加。
本研究为避免单一点测量在实验中的偶然性,选择在位移较大区域选择6个点进行数据收集,三种内固定模型的位移和活动度的对比中可见:棘突横连内固定的位移和活动度最小,而无棘突横连内固定次之,无横连的最大,因此横连和完整的棘突起到限制脊柱过度活动的作用,且横连相较于完整的棘突作用更大。在活动度的对比中可见,横连对扭转时活动度的减低明显大于其他运动状态,因此横连提供更多的扭转刚度 [22] ,同时研究发现横连也限制了前屈后伸侧屈等横向弯曲等活动 [8] 。在对3种去除内固定的脊柱模型的研究发现,切除棘突的胸腰椎在位移和活动度有2%~4%不等的增加,脊柱活动度的增加可能会造成脊柱不稳的发生,在穿过棘突放置横连和无横连的去除内固定的脊柱模型,因为影响活动的椎间盘和椎旁韧带无损坏,其位移和活动度无差异。在横连对内固定等效应力影响的研究中发现,经过棘突放置横连内固定降低了骨折临近椎体椎弓根钉的等效应力,使内固定系统更加安全,由于横连和纵棒直接相连,在运动中对纵棒有力的限制,因此纵棒的应力有小幅度的增加。
据我们所知,本研究横连放置的方式是根据术中习惯,对于切除棘突放置横连,并未采用既往全部棘突完全切除的方法 [5] [23] [24] [25] ,这种方法破坏了棘上韧带和棘间韧带,而是采用仅大于横连截面的切除,仅破坏了棘上韧带,仍保留棘间韧带的完整性。本研究为首次构建经棘突放置横连的胸腰椎爆裂骨折内固定模型,采用稍微大于横连截面的空洞,保持横连和空洞的不接触状态,并不破坏棘间韧带和棘上韧带。参考既往胸腰椎爆裂骨折建模的方式 [26] ,完全切除椎体前中柱骨质造成脊柱不稳,构建胸腰椎爆裂骨折经伤椎置钉的模型,其中伤椎椎弓根钉一半在骨质中,且和上方骨质定义为不分离。
本研究仅适用1名志愿者的胸腰椎模型进行实验,我们需要更多的健康志愿者的胸腰椎模型验证本研究的结论。本研究未模拟椎旁肌肉,椎旁肌肉有助于维持脊柱稳定性,这需要体外实验或者临床研究进一步的证实。接下来,我们将收集临床中经过上述内固定形式的骨折患者的情况,进一步证实本研究的结果。
本研究科学的证明了胸腰椎爆裂骨折经伤椎置钉固定的术式中需要经棘突放置横连,这增加了内固定的稳定性,降低了椎弓根钉的等效应力,使内固定更加安全。本发现将有助于横连在胸腰椎爆裂骨折中的应用,促进胸腰椎爆裂骨折的愈合,减少骨折不愈合和内固定失败的发生。
5. 结论
经棘突钻孔放置横连明显增加了经骨折椎骨置钉内固定治疗胸腰椎爆裂骨折中的稳定性和安全性。
NOTES
*第一作者。
#通讯作者。