摘要:
目的:探讨喉返神经“贴膜”保护技术在甲状腺癌手术中保护喉返神经(Recurrent laryngeal nerve, RLN)的临床效果。方法:回顾性分析2017年1月至2018年12月本院行甲状腺癌手术的115例患者,共有157条喉返神经被解剖并保护。按照手术日期单双号随机分配采取不同的RLN保护方法,其中:常规方法解剖保护了87条喉返神经纳入传统组(65例患者),喉返神经“贴膜”保护了70条喉返神经纳入新方法组(50例患者)。分析两组术中喉返神经电生理信号的变化以及术后患者发音情况。结果:传统组术中喉返神经电生理信号振幅下降<30%的有60例、振幅下降30%~50%的17例、振幅下降>50%的有10例;新方法组分别有64例、5例、1例;两组差异有统计学意义(P < 0.05)。传统组术后有3例出现声音嘶哑,新方法组没有声音嘶哑的病例,两组差异无统计学意义(P > 0.05)。结论:喉返神经“贴膜”保护技术有利于在甲状腺癌手术中保护喉返神经,提高了手术的安全性。
Abstract:
Objective: To investigate the clinical effect of Recurrent laryngeal nerve (RLN) “film” protection technology in thyroid cancer surgery. Methods: The study consisted of 115 patients with thyroid cancer surgery in our hospital from January 2017 to December 2018. And a total of 157 RLN were dissected and protected in the retrospective study. These patients were randomly assigned to take two different methods of RLN protection according to the date of surgery. Among them, conventional methods of anatomical protection of 87 RLN were included in the traditional group. The recurrent laryngeal nerve “film” protected 70 RLN into the new method group. The changes of electrophysiological signals of the RLN and the pronunciation of postoperative patients were analyzed. Results: In the traditional group, there were 60 cases in which the amplitude of the RLN electrophysiological signal decreased by <30%, 17 cases in which RLN signal decreased by 30% - 50%, 10 cases in which RLN signal decreased drop >50%; there were 64 cases, 5 cases, 1 case in the new method group; the difference between the two groups was statistically significant (P < 0.05). In the traditional group, 3 cases had transient hoarseness and the new method group had no hoarseness. Conclusion: The “film” protection technique of the recurrent laryngeal nerve is beneficial to the protection of the recurrent laryngeal nerve in thyroid cancer surgery and has improved the safety of the operation.
1. 引言
甲状腺癌是目前发病率增长最快的实体肿瘤,其发生率约占全身恶性肿瘤发生率的1% [1] [2] 。绝大多数甲状腺癌需要手术治疗 [3] 。甲状腺与喉返神经关系密切,喉返神经损伤是甲状腺手术的常见而且严重的并发症 [4] 。其中,热损伤是主要原因之一。单侧喉返神经麻痹患者,发音嘶哑而且易于疲劳;双侧喉返神经麻痹,导致急性吸气性呼吸困难,甚至窒息。我们与中国科学技术大学火灾科学国家重点实验室合作,研发了一种耐高温的“隔热膜”,术中贴在喉返神经表面,以减少神经热损伤,取得较好的效果,现报道如下。
2. 临床资料与方法
2.1. 一般资料
研究对象为2017年1月至2018年12月于本院行甲状腺癌手术的患者共115例,共有157条喉返神经被解剖并保护,按照手术日期单双号随机分配采取不同的RLN保护方法,常规解剖保护了87条喉返神经纳入传统组(65例患者),喉返神经“贴膜”保护了70条喉返神经纳入新方法组(50例患者)。本次研究经医院伦理委员会批准。两组患者资料比较(P > 0.05) (见表1)。
入组标准:①术前细针穿刺活检(Fine needle aspiration, FNA)诊断考虑甲状腺癌;②术中冰冻提示甲状腺癌患者;③年龄20~70岁之间,性别不限;④无甲状腺癌手术禁忌症并签署知情同意书。

Table 1. Comparison of general data between two groups of patients with thyroid cancer
表1. 两组甲状腺癌患者的一般资料比较
排除标准;①二次甲状腺癌患者;②术前声音嘶哑、喉镜检查声带运动异常的患者;;③术后常规病理证实为甲状腺良性结节患者;④术中见病灶侵犯喉返神经、喉返神经无法保留的患者;⑤侧颈部淋巴结转移患者。
2.2. 方法
传统组:采用常规的精细化操作解剖喉返神经;新技术组:沿着喉返神经走形的气管食管沟处解剖,在隐约显露神经(图1),贴着神经置入隔热膜并离断隔热膜上方组织(图2);分离RLN两侧组织(图3);全程解剖RLN并及记录其电生理信号(图4)。
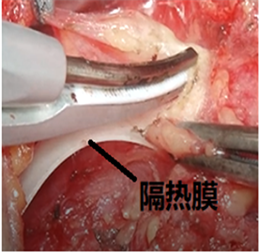
Figure 2. Disconnection of tissue above the RLN
图2. 离断喉返神经上方组织

Figure 3. Disconnection of tissue on both sides of the RLN
图3. 离断喉返神经两侧的组织
2.3. 观察指标
两组患者分别行传统法常规解剖喉返神经和新方法喉返神经“贴膜”保护解剖喉返神经,观察两种方法在术中喉返神经电生理信号振幅下降程度 [5] ;两组患者术后出现声音嘶哑的情况。
2.4. 统计学处理
采用SPSS17.0统计软件对数据进行统计分析。计量资料的比较采用t检验,计数资料的比较采用c2检验,P < 0.05为差异有统计学意义。
3. 结果
1、两组均未见甲状腺癌累及RLN且必须切除RLN的病例。传统组与新方法组甲状腺癌手术患者的术中电生理信号振幅下降>50%的发生率分别为10 (11.49%)、1 (1.43%),两组差异有统计学意义(P < 0.05) (见表2)。
4. 讨论
喉返神经损伤是甲状腺手术中的严重并发症 [4] 。据统计在大的甲状腺手术治疗中心,喉返神经损伤
Table 2. Comparison of the incidence of amplitude reduction of RLN electrophysiological signals in patients with thyroid cancer
表2. 两组甲状腺癌患者术中喉返神经电生理信号振幅下降程度发生率比较[率(%)]
2、传统组与新方法组甲状腺癌手术患者术后出现声音嘶哑情况的分别有3例、0例,差异无统计学意义(P > 0.05) (见表3)。3例声音嘶哑患者术后三个月复查,有1例发音正常,2例声带运动减弱。
Table 3. Comparison of the incidence of postoperative hoarseness in patients with thyroid cancer
表3. 两组甲状腺癌患者术后声音嘶哑发生率比较[率(%)]
的发生率在0.5%~3% [6] [7] ;单侧喉返神经麻痹患者,发音嘶哑而且易于疲劳;双侧喉返神经麻痹,导致急性吸气性呼吸困难,甚至窒息。甲状腺手术中“热损伤、过度牵拉、钳夹、缝扎、离断”等均可导致喉返神经损伤 [8] 。其中,热损伤是主要原因之一。术中电刀功率掌握不当、与神经距离太近致热灼伤,超声刀刀头工作面距离喉返神经小于5 mm以及在切割和凝固组织时产生热量及高温的小的组织碎片对神经所造成的热损伤 [9] 。我们与中国科学技术大学火灾科学国家重点实验室合作,采用多元醇、聚乙二醇等材料研发出柔性半透明防水隔热膜(已申报专利),适用于医疗手术过程中的热防护;喉返神经隔热膜保护后,距离神经2~3 mm采用超声刀或电刀操作,隔热膜背面最高温度在40℃以内。手术中隔热膜阻碍了直接的热传导,同时也避免了高温碎片及热液对喉返神经的损伤。
术中喉返神经监测技术(intraoperative neuromonitoring, IONM)目前已经较为广泛的应用于临床 [10] [11] 。通过术中电生理信号改变,我们可以及时发现喉返神经损伤程度。通常将RLN肌电信号振幅下降超过50%和潜伏期延长超过10%设置为RLN损伤的预警值 [12] ;术中信号振幅下降超过50%与术后声带运动改变存在相关性 [5] 。故本研究将振幅下降超过50%作为RLN损伤的主要评价指标。本研究发现,新方法组的术中电生理信号振幅下降超过50%的有1例(1.43%),传统组发生率分别为10 (11.49%),说明,RLN“贴膜”保护技术这一新方法减少了喉返神经损伤的发生。传统组有3例声音嘶哑患者,术后三月复查,有1例发音正常,2例声带运动减弱;新方法组没有出现声音嘶哑的病例。因遵循伦理,手术中我们在发现振幅下降后立即停止了可能损伤RLN的操作,如果术中没有采用IONM技术,可能会出现更多的RLN损伤的病例,两组差异可能会更加显著。
5. 结论
综上所述,在甲状腺癌手术中应用喉返神经保护“贴膜”保护喉返神经,对预防喉返神经损伤有较好的保护作用。我们期待着更多的临床数据以及相关的基础研究。
基金项目
喉返神经“贴膜”保护技术在甲状腺手术中的临床应用研究1604a0802073安徽省科技厅。